Cannabis in Appalachia
About Me

Appalachia is my home, with all of its wonders and flaws combined. With a deep history of exploitation, the people of the Appalachian Mountain Region have lived with higher incidences of nicotine addiction, difficulty breathing from exposure to coal dust, and limited access to both physical and mental health care. With the recent push of legalization of cannabis in the United States, I was both excited and concerned about what this may mean for the future of Appalachia. On one hand, there are many reported benefits of cannabis use for mental health (anxiety and depression), but on the other hand, what could cannabis do to further affect the quality of life and immune system health to folks often forgotten by research? To approach this double-edged research, I utilized quantitative survey methods in an attempt to measure pre-legalization cannabis use’s relationships to anxiety, depression, quality of life, and immune function.
Process
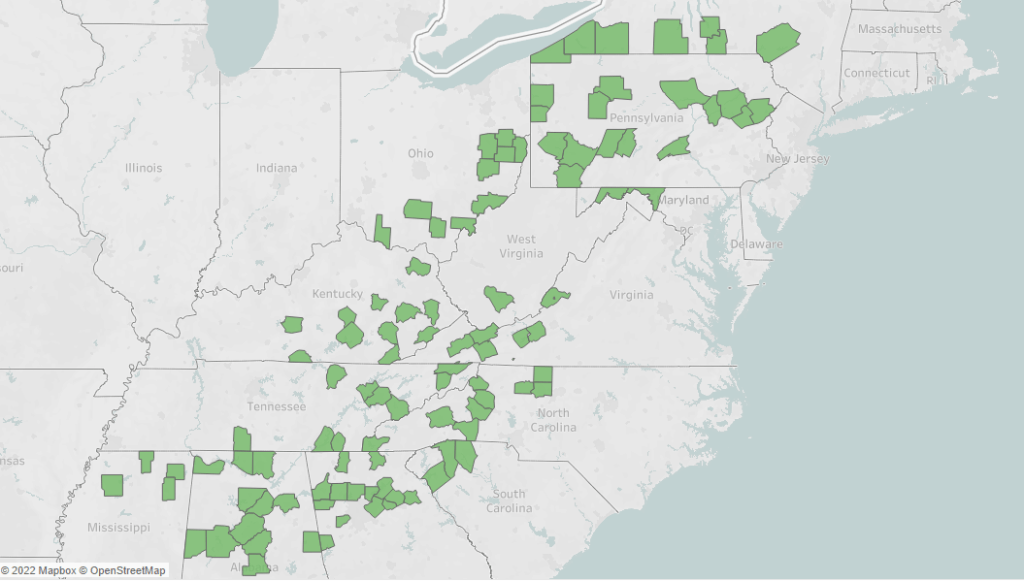
Appalachia
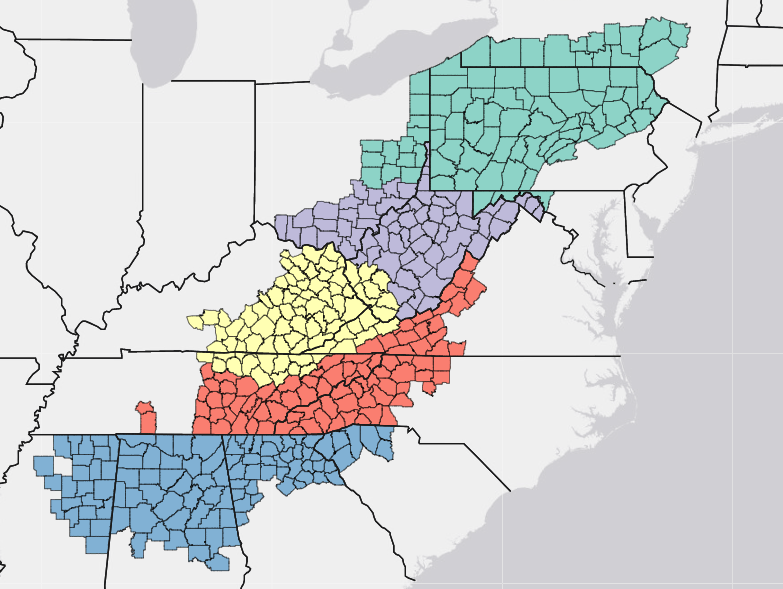
422 counties spread across 13 states along the Appalachian Mountain Chain, the Appalachia being observed is defined by the Appalachian Regional Commission. The region was once thriving with industry, albeit often with exploitative labor practices. In recent history, Appalachia has been a region rich in tradition, but often poor in economic opportunities.
Recruiting in a Time of Covid
I began the process of this dissertation research in 2020, with the ability to recruit people being limited to digital interactions for safety purposes. With this hurdle to tackle, I sought to use an online survey interface that would allow me to collect data safely for all involved and landed on SurveyMonkey.
Research Questions
In order to understand how cannabis relates currently to our measures of health and quality of life, four research questions must be asked:
- How do different levels of cannabis use relate to differences in anxiety?
- How do different patterns of cannabis use relate to scores of depression?
- Do cannabis users see difference in quality of life based on their use?
- Are cannabis users experiencing any noticeable differences in self-reported immune function?
Workflow

Two Measures of Cannabis Use
Four Scales
With four domains to observe, I chose four pre-established measures and combined them into the SurveyMonkey interface.
- Hamilton Anxiety Index (HAM-A; Hamilton, 1959)
- Patient Health Questionnaire – Depression Test (PHQ; Kroenke et al., 2001)
- CDC’s Health-Related Quality of Life measure (HRQOL; Center for Disease Control, 2000)
- Immune Status Questionnaire (ISQ; Versprille et al., 2019)
Data Collection
Recruitment
Due to the difficulty of recruiting during Covid, I was lead down the path of utilizing SurveyMonkey’s Partner Recruitment program, a wonderfully efficient, albeit expensive route to recruiting participants for surveys.
Due to limitations in the audience selection process, the study audience needed to be split in two to capture all of the counties in Appalachia (note: 250 counties were allowed per study). Two separate surveys were run in parallel to cover the entire region and were balanced on population sizes:
| Audience 1 | Audience 2 |
| Alabama | Ohio |
| Georgia | Pennsylvania |
| Kentucky | South Carolina |
| Maryland | Tennessee |
| Mississippi | Virginia |
| New York | |
| North Carolina | |
| West Virginia |

Survey Creation & My Big Mistake
Part of the difficulty of this study came about in the necessary steps to separate eligible v. ineligible participants within the states being measured. Of the 13 states included, only 1 state is completely in the Appalachian region, otherwise every state has counties that do not count and thus separating them was tedious.
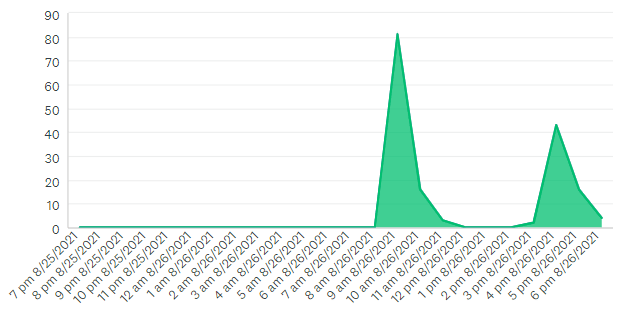
This is where I made my first mistake (see two peaks of response times). In the page logic order built into the survey, in order to separate participants by state, then county, thirteen separate pages were created that included counties for each state to avoid visual overload. Unfortunately, one of those logic pages was broken at the time the study was run, allowing many participants who did not live in Appalachia to fill out the study. SurveyMonkey customer support was swift in fixing and resolving the issue, with all data collection being completed within 12 hours.
Data Insights
Please take these results with a grain of salt, these are relationships observed in present users, for more complete understanding more research would be necessary.
Anxiety
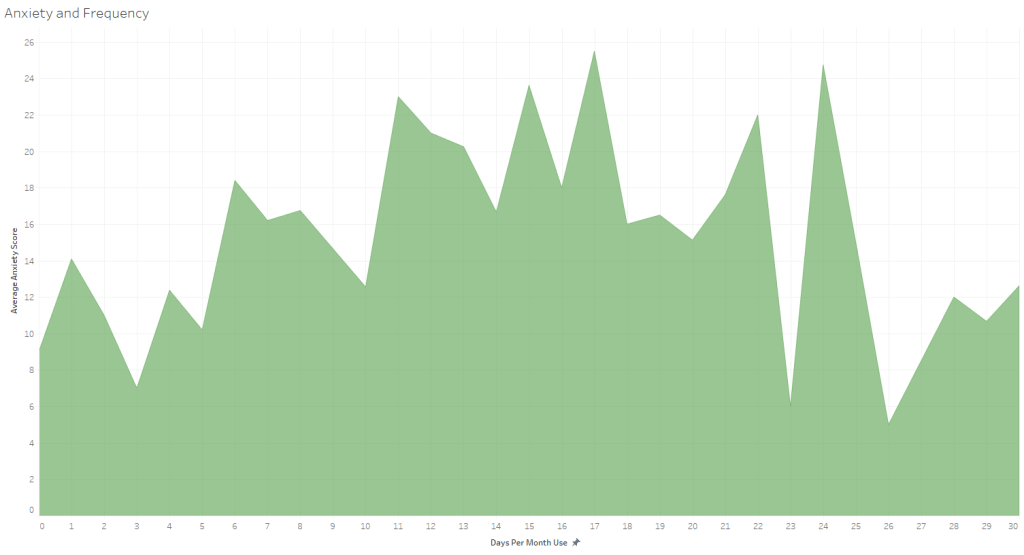
An unusual relationship was seen where anxiety was related to cannabis, but in a complex way. The study implies that those who either use very infrequently or very frequently have lower levels of anxiety compared to intermittent users.
Depression
A relationship was seen between longevity of cannabis use and depression score reductions. While a significant relationship, I personally wonder how much of the relationship is altered by a high reporting, young population who are significantly more depressed than older participants.

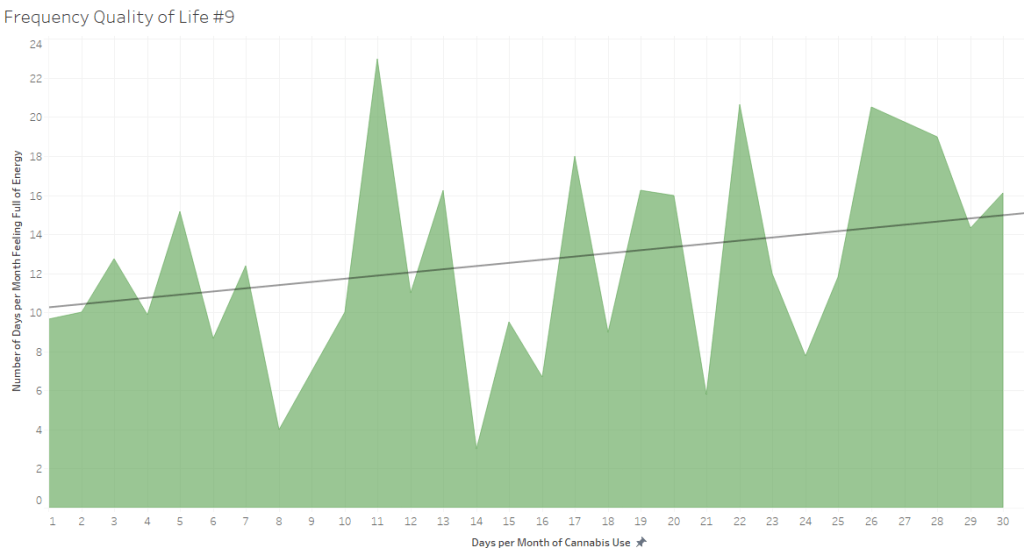
Quality of Life
Quality of Life was largely unaffected by either measure, however one relationship alluded to increased frequency of use leading to more days feeling full of energy out of the month, with averages increasing substantially.
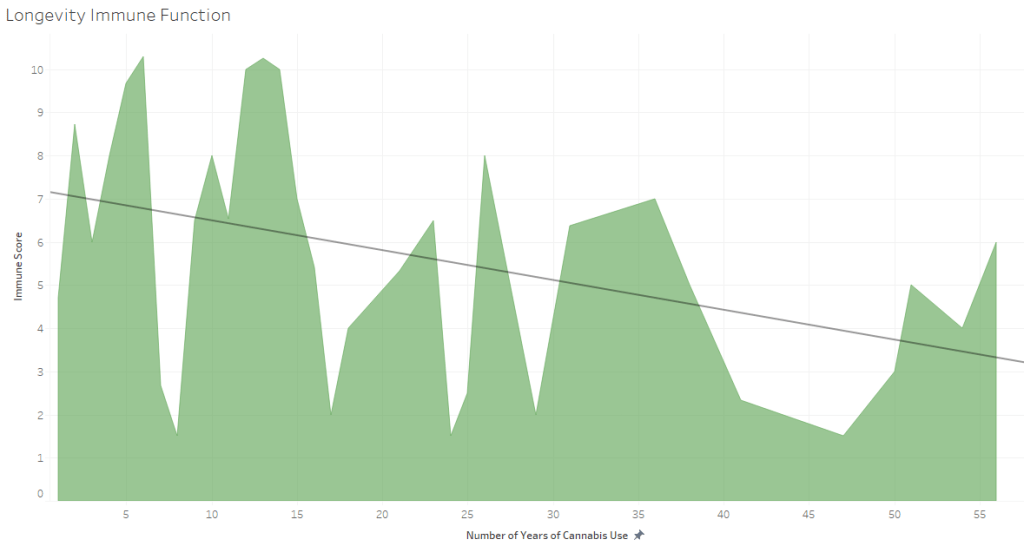
Immune Function
Immune function surprisingly improved with longevity, which is contrary to the assumption that immune function would degrade with age. NOTE: this is a measure of self-reported immune function, and as such should be considered as perspective-based.
Study Limitations
West Virginia
In the data collection process, a fair spread of the region was represented with one exception. The great and only wholly Appalachian state of West Virginia was represented by only one participant. In future iterations of the study, balancing between states would be ideal.
Budgeting
Due to this study being academic in nature, and occurring during a time full of uncertainty that caused difficulty in procuring research grants, this study was completely self-funded by me. While I was lucky to keep a full-time job throughout Covid, this was a significant cost that meant data collection could only be done once.
Second Sample
Part of the theory behind this study was to both observe the relationships that already existed, and create a data set for future observations to compare against. With federal and state cannabis legality in a place of uncertainty, having data to compare future measures to needs data to be shared safely, which lead to a significant number of steps to secure the safety and privacy of participants who were willing to share details of their illegal activity (e.g. not collecting age, rather age ranges; not collecting racial data; collecting counties rather than zip codes).
Wrap-Up
So, what did we learn?

Cannabis use has been present in Appalachia for a long time. With participants reporting having 40 and 50+ years of regular cannabis use, it should be no surprise that people will do what they want, especially when their home keeps them more hidden away from attention.
Anxiety & Depression
There does seem to be some positive and negative relationships involved with cannabis use, however nothing overwhelming or concerning.
Quality of Life
Quality of Life did not have that much involved in it outside of days of feeling good, but that does imply at least a perspective of a difference in quality of life that may be worth investigating further.
Immune Function
Immune function in relation to Cannabis use in this study missed on a major component that I believe would have a major change: route of administration. It is generally agreed upon that smoke is bad for your immune system, however with differences in method could have radically different effects on immune function (e.g. no cough from edibles, lung damage from vaping/smoking).
Overall Take Away
At least at the moment from the data collected in this study, cannabis does not seem to be a big deal. While safety is still a concern, the differences in depression and anxiety were minimal and nearly no distinctions were seen otherwise. While cannabis could still bring the same lung damage and cancer risks that tobacco did, it will take different research to determine to what extent and to further parse out any benefits.
Future Research

Differences in Routes of Administration
An investigation into the differences in anxiety, depression, quality of life, and immune function that has enough power to differentiate between users that have distinct and mixed preferred methods of consuming cannabis. (My hypothesis being that smoking/vaping would be much more negative than edibles/tinctures/teas)
Sub-Regions of Appalachia
If you ask anyone who lives in a region of Appalachia what it is likely, there will be a pretty significant difference between the regions. Pennsylvania and Mississippi feel very different, and many southern Appalachians do not even consider themselves as such. In a larger sample study, understanding the differences between patterns and methods of use between northern, central, and southern Appalachia to more personalize the public health initiatives in those regions.

Post-Legalization
It is almost limitless the possible number of studies that could be conducted if cannabis was legalized. How did different methods of action affect different mental health symptoms, what is the actual mechanism that causes a relationship between schizophrenic episodes and cannabis use, do different strains/THC profiles have significantly different actual effects on users?
A follow-up version of this study after legalization has taken place was always part of the intention of this study, to allow us to see if larger, overall patterns have changed with a different perspective on this prohibition.
